Our readiness checklist will help you assess if your practice is ready to implement Collaborative Care.
keyword: CoCM
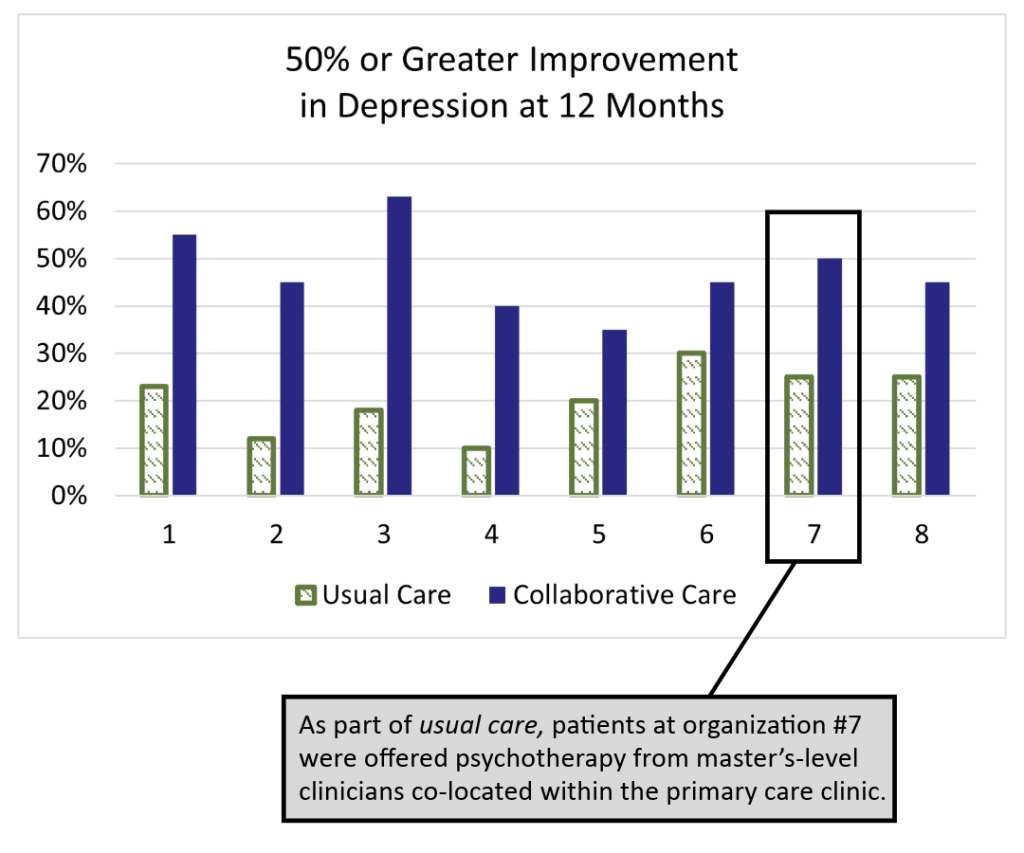
Comparing Collaborative Care to Usual Care
Introduction:
Compared with usual care, Collaborative Care has been shown to improve the effectiveness of depression treatment and lower total healthcare costs. This handout outlines those differences using data from the IMPACT trial.
A printable PDF is available for download; however, please note that this document may not conform to the WCAG-2 accessibility standards.
Comparing Collaborative Care to Usual Care
The IMPACT (Improving Mood: Providing Access to Collaborative Treatment) trial focused on depressed, older adults. Half were randomly assigned to receive the depression treatment usually offered by participating clinics, and half were randomly assigned to receive collaborative care. Collaborative care more than doubled the effectiveness of depression treatment and reduced total healthcare costs at the same time (JAMA, 2002).
Usual Care
50% of study patients used antidepressants at the time of enrollment, but were still significantly depressed.
70% of usual care patients received medication therapy from their PCP and/or a referral to specialty behavioral health.
Only 20% of patients showed significant improvements after one year, which matches national data for depression treatment in primary care.
Collaborative Care
On average, twice as many patients significantly improved. The difference was statistically significant in all eight healthcare settings. Why?
- Patient-Centered Team Care
- Population-Based Care
- Measurement-Based Treatment to Target
- Evidence-Based Care
- Accountable Care
Behavioral Health Integration Services Fact Sheet
The Centers for Medicare and Medicaid Services have an updated fact sheet detailing codes that can be used to bill for behavioral health integration (BHI) and Collaborative Care Model (CoCM) services.
Pediatric Collaborative Care Implementation Guide
This guide is for multi-disciplinary, primary care teams seeking to improve care access and behavioral health outcomes for children and adolescents through implementing Collaborative Care. Centered around the core principles of Collaborative Care, this guide serves as a roadmap to healthcare leaders, managers, clinicians, and staff in primary care as they:
- start a new Collaborative Care program, or
- expand an existing integrated care or Collaborative Care program to pediatrics, and/or
- partner with community and behavioral health agencies.
For training support and technical assistance implementing Pediatric Collaborative Care reach out to the AIMS Center at: uwaims@uw.edu. Research has shown that clinics receiving implementation support from the AIMS Center have significantly better patient outcomes.
Guidance on Verbal Patient Consent and CoCM
Ensuring that a patient understands the Collaborative Care (CoCM) program before agreeing to participate is a crucial task for primary care providers. This resource provides general guidance on obtaining verbal consent from patients to participate in CoCM. Please note that these are general tips and that specific consent requirements may vary by state and patient insurance.